Loading article
Back to Health Guides
Telehealth vs In-Person Doctor: When to Use Each
A practical decision guide for choosing remote care, a GP clinic, urgent care, or emergency help in Australia.
12 min read
·Updated 7 July 2026
·Doctor Reviewed
AHPRA Verified
In this article
- 1Start with the information the doctor needs
- 2When telehealth may fit
- 3When an in-person doctor is usually better
- 4Urgent symptoms should bypass routine telehealth
- 5The same standard still applies
Medical information only. This article is for general information and does not constitute medical advice. Treatment decisions are made by an AHPRA-registered doctor after reviewing your circumstances.
Review
InstantMed Clinical Team
Clinical governance review for guide content
Updated
7 July 2026
General information only, not personal medical advice.
Jump to section
1Start with the information the doctor needs2When telehealth may fit3When an in-person doctor is usually better4Urgent symptoms should bypass routine telehealth5The same standard still applies6Cost and speed matter after safety7How to choose the first step8What each route can and cannot collect9After telehealth, close the loop10Where each option fits11Common mistakes to avoid12Related guides13Sources Used In This Guide
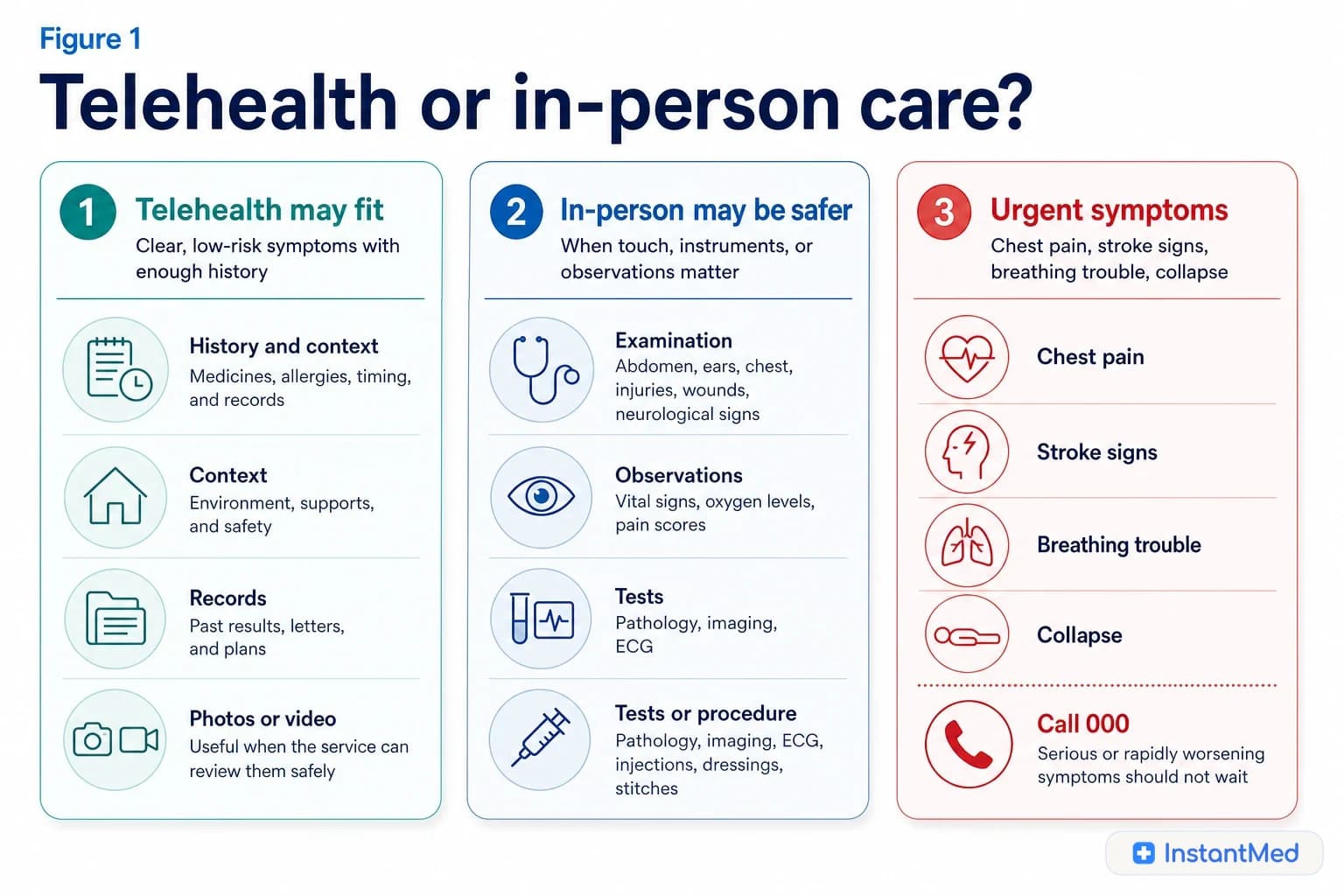
Telehealth can be the right first step when the problem can be assessed safely from a clear history, a real-time conversation, records, uploaded images, or follow-up context. In-person care is usually better when the clinician needs to examine you, take observations, arrange tests, perform a procedure, or manage a complex or urgent problem.
The practical decision is not whether telehealth is better or worse. It is whether the care route gives the clinician enough information to make a safe decision today.
Start with the information the doctor needs
A doctor can make many decisions from history: what started, when it changed, what you have tried, what medicines you take, what risks apply, and whether red flags are present. Telehealth is strongest when that information is enough.
In-person care adds physical information: examination, vital signs, oxygen level, hydration, neurological signs, abdominal tenderness, ear examination, wound depth, joint stability, pregnancy assessment, and the ability to act immediately if the situation changes.
| Clinical question | Telehealth may be enough when | In-person care is safer when |
|---|---|---|
| What is happening? | Symptoms are clear, low risk, and can be described reliably | Symptoms are new, severe, unclear, rapidly changing, or hard to describe |
| What does the doctor need to check? | History, medicines, records, photos, or video are the main evidence | Examination, observations, tests, imaging, or a procedure may change the decision |
| How quickly is care needed? | It is routine or time-sensitive but not urgent | Waiting could delay urgent treatment or monitoring |
| Who is the patient? | The patient can communicate clearly and safely | The patient is a baby, frail, pregnant with concerning symptoms, confused, very unwell, or unsupported |
| What happens next? | Advice, follow-up, remote documentation, or safe prescription review may be possible | Local clinic care, emergency care, pathology, imaging, wound care, or usual-GP review is needed |
When telehealth may fit
Telehealth works best when the problem is suitable for remote assessment and the service is willing to redirect if new information changes the risk.
Examples can include:
- a low-risk short illness where the history is clear and no urgent symptoms are present
- a repeat medicine review where the medication history, allergies, dose, monitoring, and current safety context are clear
- follow-up after a previous review when the next step can be decided from symptoms, results, or records
- a medication side-effect or interaction question where the person is stable
- review of appropriate uploaded images when the service can handle images securely and the problem does not require touch or equipment
- mental health check-ins where the person is not in immediate danger and support arrangements are clear
- triage about whether the next step should be usual GP, urgent care, emergency department, pharmacy, pathology, or imaging
The common feature is information sufficiency. Convenience is useful, but it cannot carry the clinical decision by itself.
When an in-person doctor is usually better
In-person care is stronger when the important clue is physical, the patient could deteriorate, or the care involves procedures or tests.
| Need | Why in-person helps | Examples |
|---|---|---|
| Examination | The clinician can check findings that cannot be reliably described | abdominal tenderness, ear drum, neurological signs, joint stability |
| Observations | Vital signs can change the risk category | oxygen saturation, pulse, blood pressure, temperature, hydration |
| Tests or imaging | Diagnosis may depend on objective results | urine test, blood test, ECG, X-ray, ultrasound |
| Procedures | Treatment may need equipment or hands-on care | stitches, dressings, wound cleaning, injections, vaccinations |
| Continuity | The usual doctor can integrate history over time | chronic disease, complex medicines, recurring symptoms, care plans |
| Safety escalation | The team can escalate immediately if needed | severe pain, breathing symptoms, chest symptoms, collapse, frailty |
Young children, pregnancy, frailty, disability, intoxication, confusion, language barriers without interpreter support, and unsafe home environments can lower the threshold for in-person care.
Urgent symptoms should bypass routine telehealth
Some symptoms need emergency or urgent care because delay matters. In Australia, call triple zero (000) for serious and urgent symptoms.
Use emergency care first for:
- chest pain or chest tightness
- possible stroke symptoms, such as face droop, arm weakness, speech trouble, vision change, or sudden balance problems
- severe breathing difficulty
- collapse, loss of consciousness, or a seizure
- uncontrolled bleeding
- major injury, serious assault, high fall, severe burn, poisoning, or overdose
- severe allergic reaction with breathing, throat, tongue, voice, dizziness, or collapse symptoms
- severe pain, a very unwell appearance, or symptoms that are rapidly worsening
- immediate self-harm risk or risk of harm to someone else
Healthdirect also describes virtual care clinics for some urgent but not life-threatening problems. These services are not available everywhere and may still send you to an emergency department, clinic, ambulance, pathology, or imaging if virtual review is not safe enough.
The same standard still applies
Telehealth changes the channel, not the clinical duty. A safe telehealth consultation still needs identity checks, consent, privacy, adequate history, records, secure handling of information, and a plan for what happens if the technology fails or the patient needs in-person care.
Figure 2
Remote care and clinic care collect different evidence. The best first step is the one that can check the thing that matters.
This is why a good telehealth service may ask follow-up questions, request more information, decline a request, or recommend a different care route. That friction can be protective.
Cost and speed matter after safety
Speed and price are real considerations, but they should not be the first filter.
Australian care can involve several billing models:
- an in-person GP clinic may bulk bill, mixed bill, or charge a private fee
- a regular GP may offer Medicare-funded telehealth when eligibility rules are met
- a private telehealth service may charge an out-of-pocket fee
- urgent care clinics, public hospital emergency departments, and virtual care services can have different access and billing rules depending on the state, eligibility, and setting
Ask two questions in this order:
- 1
Which care route can assess this safely?
- 2
What will that specific service cost, how soon can it help, and what happens if it redirects me?
A cheap or fast consultation is poor value if the problem actually needs examination, tests, monitoring, or emergency care. An in-person booking is also not automatically better if the issue is suitable for safe remote review and access is the main barrier.
How to choose the first step
| Situation | Better first step | Why |
|---|---|---|
| Serious, sudden, or rapidly worsening symptoms | 000 or emergency department | Treatment, monitoring, ambulance support, or urgent imaging may be needed |
| Urgent but not life-threatening symptoms | Urgent care clinic, after-hours GP, or state virtual care where available | Same-day triage, observations, tests, or escalation may be needed |
| Clear low-risk issue with no red flags | Telehealth may fit | A clinician may be able to decide from history, records, images, or video |
| Routine short illness evidence | Telehealth may fit if assessment is adequate | The decision may be history-based when no red flags are present |
| Stable repeat medicine review | Telehealth may fit if medicine history is clear | Safety checks can sometimes be done remotely |
| New undiagnosed symptom | GP clinic often fits better | Examination or tests may be needed before treatment |
| Injury, wound, severe pain, or possible fracture | GP, urgent care, or emergency depending on severity | Physical assessment, imaging, dressing, stitches, or procedure may be needed |
| Chronic disease or complex medicines | Usual GP or specialist | Continuity, monitoring, interactions, and trend data matter |
| Unsure where to go | Healthdirect 1800 022 222 or Symptom Checker | Triage can help choose GP, urgent care, pharmacy, telehealth, or emergency |
What each route can and cannot collect
| Information type | Telehealth can collect | In-person care can collect |
|---|---|---|
| Symptom history | Yes | Yes |
| Medication list and allergies | Yes | Yes |
| Uploaded photos or documents | Sometimes, if privacy-safe and clinically appropriate | Yes, plus direct viewing |
| Video observation | Sometimes | Yes, direct observation |
| Touch-based examination | No | Yes |
| Vital signs | Only if the patient has reliable readings or devices | Yes |
| Pathology or imaging | Can request or refer when appropriate | Can request, collect in some settings, or coordinate locally |
| Procedures and wound care | No | Yes |
| Emergency monitoring | No | Yes, in urgent or hospital settings |
After telehealth, close the loop
Telehealth is safest when it connects back to the rest of your care. After a remote consultation, keep the advice, document, prescription token, referral, or test request somewhere you can find it. Share important outcomes with your regular GP when clinically relevant.
If a prescription is issued electronically, the Australian Digital Health Agency explains that an eScript token can be sent by SMS or email and taken or forwarded to a pharmacy. That does not remove the clinical prescribing checks. It only changes how the prescription reaches the pharmacy.
If symptoms worsen after a telehealth consultation, do not wait for the same route to reply. Use the escalation advice you were given, contact Healthdirect, see an in-person clinician, or use emergency care if symptoms become serious.
Where each option fits
Decision guide
Choose the care route that has enough information
May fit telehealth
- The problem is low risk, the history is clear, urgent symptoms are absent, and the doctor can ask follow-up questions.
- Records, photos, video, medication history, or recent results provide enough information for a safe decision.
Needs in-person care
- Examination, observations, tests, imaging, procedures, immunisations, complex medicine changes, pregnancy assessment, or usual-GP continuity may change the plan.
- The patient is very young, frail, confused, unsupported, unable to communicate safely, or symptoms are new and unclear.
Urgent care
- Serious, sudden, or worsening symptoms should bypass routine telehealth and routine GP booking.
- Use 000 for emergencies, or a local urgent care pathway when same-day assessment is needed but it is not immediately life-threatening.
Figure 3
A safe service redirects when remote review is not enough, and emergency symptoms should not wait for routine care.
Common mistakes to avoid
- 1
Choosing telehealth because it is convenient when the symptom clearly needs examination.
- 2
Assuming every in-person appointment is automatically safer, even for simple remote-suitable questions.
- 3
Treating a telehealth decline as a customer-service problem rather than a clinical boundary.
- 4
Focusing on cost before deciding whether the route is clinically suitable.
- 5
Forgetting to share important remote-care outcomes with the usual GP.
- 6
Waiting for routine telehealth when symptoms are severe or getting worse.
Related guides
- Telehealth vs GP: what is actually different in Australia?
- When telehealth cannot help
- Is telehealth safe in Australia?
- Emergency vs telehealth: when to go to ED
Sources Used In This Guide
- Australian Government Department of Health, Disability and Ageing: Telehealth
- Medical Board of Australia: Telehealth consultations with patients
- Australian Digital Health Agency: Telehealth
- Healthdirect: Hospital emergency departments
- Healthdirect: Virtual care clinics
- Healthdirect: The role of a GP
Frequently Asked Questions
Is telehealth as good as seeing a doctor in person?
It can be the right care route for suitable issues, but it is not interchangeable with in-person care. The safer question is whether the clinician has enough information to assess the problem remotely, or whether examination, observations, tests, procedures, continuity, or urgent treatment are needed.
When should I choose in-person care first?
Choose in-person care first when the decision may depend on hands-on examination, vital signs, oxygen level, wound care, imaging, pathology, vaccination, a procedure, pregnancy assessment, a young child, frailty, complex chronic disease, or symptoms that are severe, new, unclear, or worsening.
When can telehealth be a reasonable first step?
Telehealth may be reasonable when the issue is low risk, the history is clear, urgent symptoms are absent, and the clinician can make a safe decision using conversation, records, uploaded images, medication history, or follow-up information.
What if telehealth says I need to be seen in person?
Follow that advice. A redirect to a GP clinic, urgent care clinic, emergency department, pathology, imaging, pharmacy, or your usual doctor means the remote channel did not provide enough information for a safe decision.
Can telehealth help with prescriptions?
Sometimes. Prescribing still requires an appropriate clinical assessment, safe medication history, jurisdiction rules, and arrangements for receiving the prescription. It may be declined or redirected when monitoring, examination, usual-GP context, or urgent care is needed.
Should I use telehealth for emergency symptoms?
No. Chest pain, stroke symptoms, severe breathing difficulty, collapse, seizure, severe allergic reaction, uncontrolled bleeding, major injury, poisoning, overdose, or immediate self-harm risk should bypass routine telehealth. Call triple zero (000) for serious and urgent symptoms.
InstantMed Medical Team
Related Articles

11 min read
Telehealth vs GP: What's Actually Different in Australia?
Telehealth and in-person GP care are not rivals. Telehealth can be useful for suitable remote assessment, while GP clinics remain essential for examination, continuity, procedures, tests, and complex care.
InstantMed Medical Team

11 min read
When Telehealth Cannot Help: Knowing the Limits
Telehealth can be safe and useful when the problem fits remote assessment. It cannot replace emergency care, a physical examination, monitoring, or continuity when those are needed. This guide explains the limits and safer next steps.
InstantMed Medical Team

11 min read
Is Telehealth Safe in Australia?
Telehealth can be safe when the service is regulated, the doctor has enough information, and there is a clear path to in-person or urgent care when remote review is not enough.
InstantMed Medical Team