Loading article
Back to Health Guides
Chest Infections and Antibiotics: When Online Assessment Is Appropriate
Most acute bronchitis is viral. Pneumonia, severe breathlessness, oxygen concerns, and high-risk patients need in-person assessment.
8 min read
·Updated 10 May 2026
·Doctor Reviewed
AHPRA Verified

In this article
- 1What People Mean By Chest Infection
- 2Bronchitis, Pneumonia And Flares Need Different Decisions
- 3Why Antibiotics Often Do Not Help
- 4When Pneumonia Becomes The Concern
- 5What Telehealth Can Assess
Medical information only. This article is for general information and does not constitute medical advice. Treatment decisions are made by an AHPRA-registered doctor after reviewing your circumstances.
Review
InstantMed Clinical Team
Clinical governance review for guide content
Updated
10 May 2026
General information only, not personal medical advice.
Jump to section
1What People Mean By Chest Infection2Bronchitis, Pneumonia And Flares Need Different Decisions3Why Antibiotics Often Do Not Help4When Pneumonia Becomes The Concern5What Telehealth Can Assess6Information That Makes A Remote Review Safer7When Online Antibiotic Assessment May Be Reasonable8When In-Person Care Is Safer9What A Safe Review Plan Should Include10What Helps While A Viral Chest Infection Settles11The Bottom Line12Sources Used In This Guide
Key Information
A chesty cough does not automatically mean antibiotics are needed. The safest first question is whether the symptoms suggest simple viral bronchitis, possible pneumonia, or a breathing problem that needs in-person assessment.
"Chest infection" is a broad phrase. Patients use it to describe cough, phlegm, chest tightness, wheeze, fever, and feeling generally unwell. Clinically, those symptoms can come from several different problems, and the treatment is not the same.
The biggest mistake is assuming coloured phlegm means bacteria. It often does not.
The second mistake is assuming telehealth can safely sort every chest symptom. It cannot. Some lower-risk cough and infection patterns can be assessed remotely, but pneumonia and significant breathing symptoms need examination, observations, and sometimes imaging.
What People Mean By Chest Infection
Chest infection usually refers to infection affecting the lower respiratory tract: the larger airways or the lung tissue.
| Condition | What it means | Antibiotics? |
|---|---|---|
| Acute bronchitis | Inflamed airways, usually after a viral infection | Usually no in otherwise healthy adults |
| Pneumonia | Infection involving the lung tissue | Often yes, but usually needs in-person assessment |
| COPD flare | Worsening symptoms in someone with COPD | Sometimes, depending on sputum, breathlessness, and severity |
| Post-viral cough | Cough after the infection is settling | No, unless the picture changes |
Healthdirect describes chest infections as common and notes that treatment depends on the cause. Therapeutic Guidelines and antimicrobial stewardship resources consistently distinguish viral bronchitis from bacterial pneumonia and higher-risk lower respiratory infections.
Bronchitis, Pneumonia And Flares Need Different Decisions
The practical decision is not "antibiotics or no antibiotics". It is whether the story fits a lower-risk airway infection, possible lung-tissue infection, deterioration of an existing lung condition, or a non-infectious cause of chest symptoms.
| Pattern | Typical decision point | Why it matters |
|---|---|---|
| Acute bronchitis | Is this a viral cough illness without pneumonia features? | Antibiotics usually add harm without benefit in otherwise healthy adults |
| Pneumonia concern | Are fever, breathlessness, chest pain, frailty, or oxygen concerns present? | Examination, observations, and sometimes chest X-ray may be needed |
| Asthma deterioration | Is wheeze, reliever use, or poor response escalating? | The priority may be asthma action-plan care, not antibiotics |
| COPD flare | Has sputum, breathlessness, or baseline function changed? | Some flares need antibiotics, steroids, oxygen assessment, or urgent review |
| Cardiac or clot concern | Is chest pain, collapse, leg swelling, or sudden breathlessness present? | Do not label serious non-infectious problems as a chest infection |
Why Antibiotics Often Do Not Help
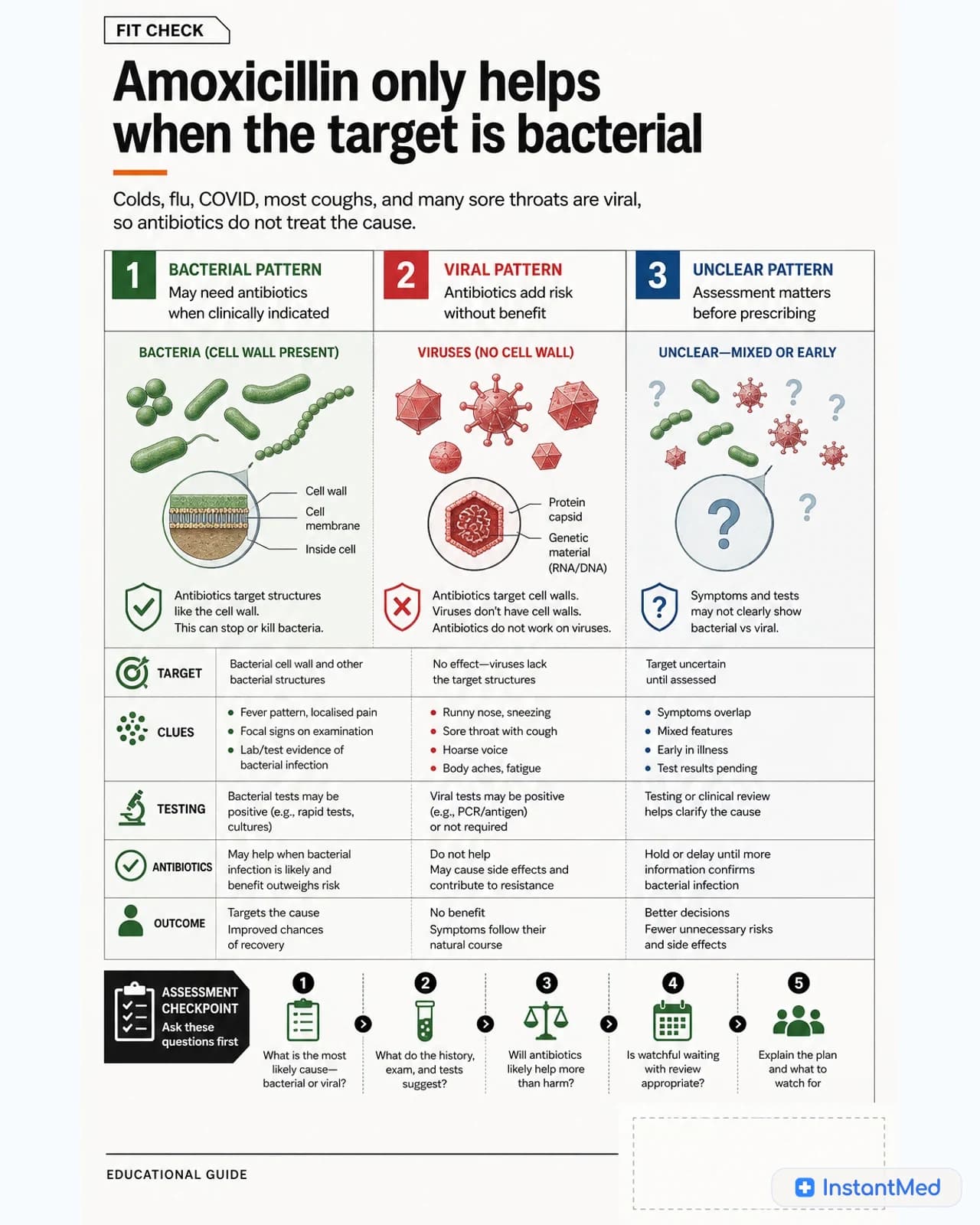
Many acute cough illnesses are viral. Antibiotics do not treat viruses.
Viral bronchitis can still feel dramatic:
- Deep cough
- Yellow or green sputum
- Chest tightness
- Fatigue
- Low-grade fever
- Wheeze or noisy breathing
- Cough lasting two to three weeks, sometimes longer
That symptom list can sound bacterial, but sputum colour is not enough. Yellow or green phlegm often reflects immune activity and airway inflammation.
Antibiotics used when they are not needed can cause diarrhoea, rash, thrush, allergy, medication interactions, and antimicrobial resistance. The Australian Commission on Safety and Quality in Health Care has a patient decision aid specifically about acute bronchitis and antibiotic use because this is such a common overprescribing area.
When Pneumonia Becomes The Concern
Pneumonia is more serious than ordinary bronchitis. It can be bacterial, viral, or mixed, and bacterial pneumonia often needs antibiotics. The issue is that pneumonia is not something telehealth can confidently rule out when symptoms are moderate or severe.
Symptoms that raise concern include:
- High fever or shaking chills
- Shortness of breath at rest or with minimal activity
- Sharp chest pain that worsens when breathing
- Confusion, drowsiness, or severe weakness
- Fast breathing
- Oxygen saturation concerns if you have a pulse oximeter
- Symptoms that are worsening rather than gradually improving
- Older age, pregnancy, immune suppression, COPD, heart failure, or significant chronic disease
In-person assessment can include respiratory rate, oxygen saturation, chest examination, blood pressure, pulse, temperature, and sometimes chest X-ray. Those details matter.
Important Warning
Call 000 for severe breathlessness, blue lips or skin, confusion, collapse, severe chest pain, or rapid deterioration. Do not wait for an online review when breathing or circulation may be compromised.
What Telehealth Can Assess
Telehealth can be useful for lower-risk respiratory symptoms when the main task is history-taking and safety screening.
A clinician may assess:
Common myth
Doctors look at the full pattern: fever, breathlessness, severity, duration, risk factors, and deterioration.
- When the cough started
- Whether symptoms are improving, static, or worsening
- Fever pattern and severity
- Breathlessness and ability to speak normally
- Chest pain type
- Sputum amount and change from baseline
- Wheeze or asthma symptoms
- Smoking history
- COPD, asthma, bronchiectasis, heart disease, diabetes, or immune risk
- Recent COVID, flu, RSV, or household illness
- Recent antibiotics
- Medication allergies
Telehealth cannot directly listen to the chest, measure oxygen saturation unless you have a reliable reading, or arrange immediate imaging during the consultation. That is why good remote care has a low threshold for referral when symptoms suggest pneumonia or significant breathing risk.
Information That Makes A Remote Review Safer
If you are seeking advice remotely, the useful details are concrete. "Chest infection" is less helpful than a timeline of what changed.
Before assessment, note:
- Day symptoms started and whether they are improving, static, or worsening
- Highest measured temperature and whether fever is persistent
- Whether you are breathless while resting, walking, climbing stairs, or speaking
- Chest pain location and whether it worsens with breathing, coughing, or exertion
- Wheeze, asthma reliever use, COPD baseline, or known lung disease
- Sputum amount and whether it is new compared with your usual baseline
- COVID, influenza, RSV, or household exposure information if known
- Oxygen saturation if you own a reliable pulse oximeter and know your usual baseline
- Pregnancy, older age, immune suppression, heart disease, diabetes, or frailty
- Recent antibiotics, allergy history, and current medicines
These details do not guarantee remote treatment. They help the clinician decide whether remote care is reasonable or whether the safer next step is in-person assessment.
When Online Antibiotic Assessment May Be Reasonable
Remote antibiotic assessment may be reasonable when:
- The patient is an adult
- Symptoms are lower risk
- Breathlessness is mild or absent
- There are no emergency symptoms
- The history strongly suggests bacterial infection or a COPD flare where antibiotics may be indicated
- The clinician has enough allergy, medicine, and risk-factor information
- There is a clear review plan if symptoms worsen
Even then, antibiotics are not guaranteed. The clinician may recommend symptomatic care, testing, an in-person GP review, urgent care, or emergency care depending on the pattern.
When In-Person Care Is Safer
Use in-person care rather than remote-only review for:
- Suspected pneumonia
- Breathlessness at rest
- Oxygen saturation below your usual level or below normal
- High fever with rigors or severe weakness
- Chest pain that is sharp, severe, crushing, or unexplained
- Symptoms in older adults with frailty or multiple conditions
- Pregnancy
- Children
- Immunocompromised patients
- COPD with severe symptoms or low oxygen
- Asthma symptoms not responding to reliever treatment
- Symptoms not improving after expected timeframes
- A second worsening after initial improvement
Being sent for in-person care is not a failure. It is the right safety boundary.
What A Safe Review Plan Should Include
For lower-risk symptoms managed outside hospital, the plan should explain what to monitor. A useful plan names the expected recovery pattern, what would make the diagnosis less likely, and when to seek care.
For example, a viral bronchitis plan should not promise overnight recovery. Cough can linger even after the infection is improving. The important question is whether fever, breathlessness, chest pain, or general illness is worsening rather than gradually settling.
Urgent signs
Severe breathlessness, blue lips, confusion, collapse, severe chest pain, or rapid deterioration need emergency care.
If antibiotics are prescribed because a bacterial pattern is plausible, the plan should still include a safety net: when improvement should begin, what side effects matter, what to do if breathing worsens, and when testing or in-person review is needed.
What Helps While A Viral Chest Infection Settles
For many viral chest infections, treatment is supportive:
- Rest and fluids
- Avoid smoking and vaping
- Use fever or pain relief if suitable for you
- Honey may ease cough in adults and children over one year old
- Use asthma or COPD medicines as prescribed if you have those conditions
- Monitor breathing, fever, and energy
- Seek review if symptoms worsen or do not follow the expected recovery pattern
Do not use leftover antibiotics. Do not borrow someone else's antibiotics. Do not buy antibiotics from online sellers that avoid proper prescribing.
The Bottom Line
Telehealth can help assess some lower-risk chest infection symptoms, but chest symptoms need a stricter safety boundary than many other online requests.
Most acute bronchitis is viral and does not need antibiotics. Pneumonia, significant breathlessness, high fever with systemic illness, older age, pregnancy, immune risk, COPD severity, and oxygen concerns need in-person assessment.
The right outcome is not always an antibiotic. The right outcome is matching the symptom pattern to the safest channel of care.
Sources Used In This Guide
- Healthdirect Australia: chest infection, cough, bronchitis, and pneumonia information
- Therapeutic Guidelines: acute bronchitis and pneumonia guidance
- Australian Commission on Safety and Quality in Health Care: acute bronchitis antibiotic decision aid and antimicrobial stewardship
- RACGP: respiratory infection and persistent cough guidance
Frequently Asked Questions
Can telehealth diagnose pneumonia?
Telehealth cannot confirm or safely exclude pneumonia with the same confidence as in-person assessment. Pneumonia may need chest examination, oxygen saturation measurement, and sometimes chest X-ray. Symptoms such as significant breathlessness, high fever, chest pain with breathing, confusion, or severe illness need in-person or urgent care.
Do chest infections always need antibiotics?
No. Many chest infections, especially acute bronchitis, are viral and do not improve with antibiotics. Antibiotics are used when bacterial infection is likely and the benefit outweighs the risks.
Does green or yellow phlegm mean I need antibiotics?
No. Coloured sputum can happen with viral bronchitis and does not prove bacterial infection. Doctors look at the whole pattern: severity, fever, breathlessness, risk factors, duration, examination findings where available, and deterioration.
When should chest infection symptoms be urgent?
Call 000 or seek urgent care for severe breathlessness, blue lips or skin, confusion, collapse, chest pain that may be cardiac, oxygen concerns, or rapid deterioration. Telehealth is not the right channel for these symptoms.
Can antibiotics be prescribed online for a chest infection?
Sometimes, but only when the presentation is lower risk, the history gives enough information, and antibiotics are clinically appropriate. If pneumonia, severe illness, high-risk patient factors, or the need for examination is present, in-person care is safer.
InstantMed Medical Team
Related Articles
8 min read
Amoxicillin in Australia: Uses, Dosing, and What to Know
Amoxicillin is a penicillin antibiotic used for selected bacterial infections. It does not treat viruses, and the right dose depends on the infection, person, and clinical context.
InstantMed Medical Team

8 min read
When Antibiotics Are Appropriate: Bacterial vs Viral Infections
Antibiotics treat bacterial infections, not viruses. This guide explains when antibiotics may be appropriate, when they are usually avoided, and what responsible use looks like.
InstantMed Medical Team
9 min read
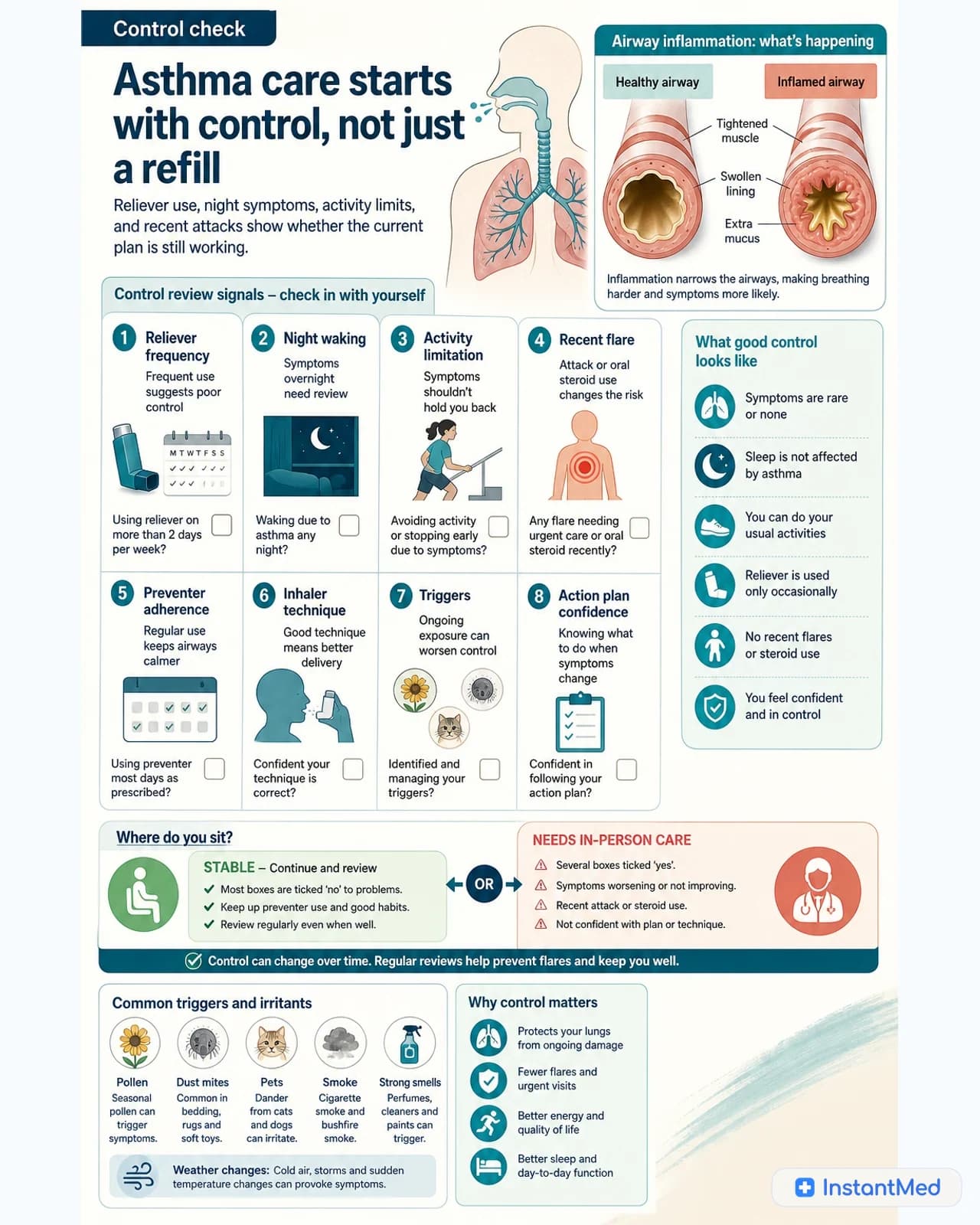
Asthma Management and Telehealth in Australia
Stable, established asthma may suit telehealth medication review, but diagnosis, worsening symptoms, children, and asthma attacks need in-person or emergency care. Learn the safety boundaries.
InstantMed Medical Team