Loading article
Back to Health Guides
Asthma Management and Telehealth in Australia
When remote asthma review may be appropriate, when symptoms need in-person care, and why an action plan matters.
9 min read
·Updated 10 May 2026
·Doctor Reviewed
AHPRA Verified
In this article
- 1What Telehealth Can and Cannot Do for Asthma
- 2Asthma Medications Available via Telehealth
- 3What The Doctor Reviews
- 4Control Questions That Matter
- 5PBS Costs for Asthma Medications
Medical information only. This article is for general information and does not constitute medical advice. Treatment decisions are made by an AHPRA-registered doctor after reviewing your circumstances.
Review
InstantMed Clinical Team
Clinical governance review for guide content
Updated
10 May 2026
General information only, not personal medical advice.
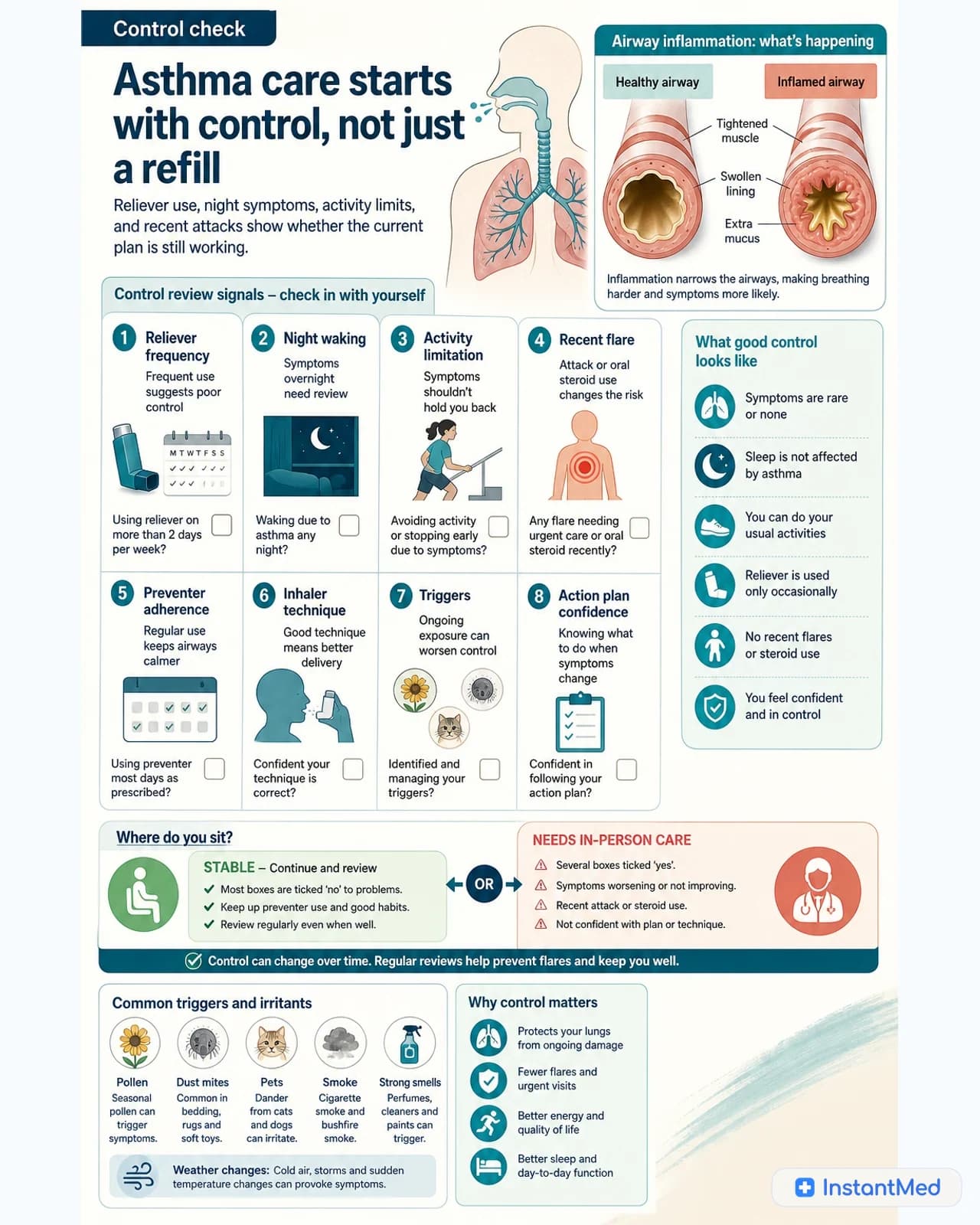
Asthma affects approximately 2.8 million Australians, making it one of the most common chronic conditions in the country. For people with stable, established asthma, some routine medication review can happen remotely. But asthma is not just an inhaler supply problem. Reliever use, night symptoms, activity limitation, recent attacks, and action-plan confidence all show whether the current plan is safe.
This guide covers what telehealth can and cannot do for asthma management, what requires in-person care, and when asthma symptoms should bypass telehealth entirely.
Important Warning
If you are having an acute asthma attack that is not responding to your reliever inhaler, do not seek telehealth care. Call 000 or go to the nearest emergency department immediately.
What Telehealth Can and Cannot Do for Asthma
Understanding the boundary matters. Telehealth is appropriate for some asthma care and not others.
May be appropriate for telehealth:
- Medication review for stable, previously diagnosed asthma
- Discussion of reliever use, preventer adherence, triggers, and action-plan confidence
- Repeat prescribing where the existing plan remains appropriate
- Referral letters for specialist review when needed
Requires in-person assessment:
- First-time asthma diagnosis (spirometry required)
- Significantly worsening asthma control
- Stepping up treatment to a higher tier (e.g., adding a LABA or LAMA)
- Oral corticosteroid prescribing for acute exacerbation
- Any features suggesting anaphylaxis, vocal cord dysfunction, or another diagnosis
- Children under 12 with asthma symptoms
The key principle: if your asthma is stable and your current treatment is working, telehealth may be suitable for routine review. If things have changed, worse control, more frequent reliever use, new symptoms, or recent attacks, an in-person review is the safer choice.
Asthma Medications Available via Telehealth
Reliever Inhalers (Short-Acting Beta-Agonists)
Reliever inhalers are used for immediate symptom relief. They work by relaxing the muscles around the airways, opening them quickly during an episode of wheeze, chest tightness, or breathlessness.
Salbutamol (Ventolin, Asmol, Salamol): The most commonly prescribed reliever in Australia. PBS-listed. Can be prescribed via telehealth for established asthma patients.
Terbutaline (Bricanyl): An alternative SABA, also PBS-listed and prescribable via telehealth.
If you are using your reliever inhaler more than twice per week (outside of exercise), your asthma may not be optimally controlled. This warrants review and may need in-person assessment if treatment needs to change.
Preventer Inhalers (Inhaled Corticosteroids and Combinations)
Preventer inhalers reduce airway inflammation over time and are taken daily, regardless of symptoms. They are the cornerstone of moderate to severe asthma management under the National Asthma Council Australia guidelines.
Inhaled corticosteroids (ICS):
- Fluticasone propionate (Flixotide)
- Budesonide (Pulmicort)
- Beclometasone (Qvar)
- Ciclesonide (Alvesco)
ICS/LABA combinations (preventer + long-acting reliever):
- Fluticasone/salmeterol (Seretide)
- Budesonide/formoterol (Symbicort, Breyna)
- Fluticasone/vilanterol (Breo Ellipta)
- Fluticasone/formoterol (Flutiform)
Many preventer inhalers are PBS-listed for established asthma. For patients already stable on one of these medications, telehealth review may be clinically appropriate if no red flags or control concerns are present.
Maintenance and Reliever Therapy (MART)
The MART approach uses a single ICS/LABA combination inhaler (specifically budesonide/formoterol formulations) as both the daily preventer and the as-needed reliever. This is a recommended strategy in current Australian asthma guidelines for eligible patients. Telehealth is appropriate for prescribing MART continuation in patients already established on this regimen.
What The Doctor Reviews
A telehealth doctor prescribing asthma medication will assess:
Asthma control: How often you are using your reliever, whether symptoms are waking you at night, whether asthma is limiting your daily activities. Poorly controlled asthma generally requires an in-person medication review rather than a simple repeat script.
Current treatment and adherence: Which medications you are currently prescribed, whether you are taking them as directed, and whether your inhaler technique has been checked recently.
Recent changes: Any new symptoms, recent respiratory illnesses, changes in exercise tolerance, or new triggering factors.
Prescription history: How long you have been on the current regimen and whether the most recent prescription was from a treating GP who has your full clinical history.
Red flags: Any features suggesting the diagnosis is not straightforward asthma, or that something more significant is happening (e.g., significant unintentional weight loss, haemoptysis, cardiac symptoms).
If the assessment is straightforward, routine prescribing may be appropriate. If anything suggests a medication change is needed or that asthma control is deteriorating, the doctor should recommend an in-person review rather than simply continue the existing plan.
Control Questions That Matter
The National Asthma Council describes poor current asthma control as symptoms or reliever use on more than 2 days per week, night symptoms or waking, or activity limitation during the previous 4 weeks.
Practical review questions include:
Telehealth boundary
Repeat medicine review can be remote for some established patients; diagnosis, deterioration, and children need in-person care.
- How many days per week do you have daytime symptoms?
- Are you waking at night or coughing on waking?
- How often are you using a reliever, excluding planned use before exercise?
- Are symptoms limiting exercise, work, study, or sleep?
- Have you had an asthma attack, urgent visit, hospital care, or oral steroids recently?
- Do you have an up-to-date action plan?
- Has your inhaler technique been checked recently?
- Are you taking preventer treatment as directed?
If several answers suggest poor control, the issue is not just access to another inhaler. The plan may need review, triggers may need attention, inhaler technique may be wrong, or another diagnosis may need to be considered.
PBS Costs for Asthma Medications
Many commonly prescribed asthma medications are PBS-listed in Australia when prescribed for eligible indications.
From 1 January 2026, before the PBS Safety Net:
- General patients pay up to $25 for most PBS medicines.
- Concession card holders pay up to $7.70.
- The 2026 PBS Safety Net thresholds are $1,748.20 for general patients and $277.20 for concession card holders.
- After reaching the threshold, general patients generally pay the concessional rate and concession card holders may receive eligible PBS medicines at no charge.
These figures apply to PBS-listed medicines and eligible patients. Private prescriptions, non-PBS medicines, brand premiums, delivery, and pharmacy-specific charges can change the final amount.
Key Information
The PBS subsidy is attached to the medication, not how the prescription was obtained. A telehealth eScript attracts the same PBS pricing as a script from your in-person GP. You pay the standard co-payment at any Australian pharmacy.
Asthma Action Plans
A written Asthma Action Plan tells you what to do when your asthma worsens - which medications to take, at what dose, and when to seek emergency care. The National Asthma Council recommends all people with asthma have an up-to-date written plan.
Your Asthma Action Plan should be reviewed whenever your treatment changes and at least annually. While a telehealth doctor can discuss your current plan and note any issues, a comprehensive plan review is best done with your regular GP who has your full history and can perform peak flow assessment in person.
When to Call 000
Asthma can be life-threatening. Go to emergency immediately if:
- Your reliever inhaler is not improving symptoms after 4 puffs and 4 minutes
- You cannot complete a full sentence due to breathlessness
- Your lips, fingertips, or tongue are turning blue (cyanosis)
- You are working very hard to breathe (ribs visible during breathing)
- Your peak flow is below 50% of your personal best
- You feel unusually anxious, confused, or exhausted from breathing
Emergency signs
Reliever not helping, trouble speaking, blue lips, exhaustion, or rapidly worsening breathing needs emergency care.
None of these presentations are appropriate for telehealth. Call 000 or get to the nearest emergency department.
The Bottom Line
Telehealth can work well for stable, established asthma where the treatment plan is unchanged and the review confirms control is good. It does not replace the respiratory assessment, spirometry, inhaler-technique check, or in-depth management review that in-person care provides.
If your asthma symptoms have changed, your control is worsening, you are using reliever medicine more often, or you have never been formally diagnosed, see your GP or a respiratory specialist in person.
Sources
- AIHW: Asthma in Australia
- National Asthma Council Australia: How is asthma managed?
- Australian Asthma Handbook: Assessing and reviewing asthma in adults and adolescents
- National Asthma Council Australia: Asthma first aid
- Better Health Channel: Asthma emergency first aid
- Services Australia: PBS Safety Net thresholds
- PBS: About the PBS
Frequently Asked Questions
Can asthma medication be reviewed through telehealth?
Sometimes. Telehealth may be appropriate for stable, previously diagnosed asthma where the person is established on a treatment plan. It is not appropriate for a first diagnosis, severe symptoms, rapidly worsening control, or an acute asthma attack.
Can preventer inhalers be reviewed through telehealth?
For some established patients, yes. A doctor still needs to review asthma control, recent symptoms, reliever use, adherence, and whether the current treatment remains appropriate. Worsening control often needs in-person review.
When do I need to see a doctor in person for asthma?
You should attend an emergency department immediately if your reliever inhaler is not working, you cannot complete a full sentence, your lips or fingernails are turning blue, or your breathing is worsening rapidly. For uncontrolled asthma, new symptoms, or a first-time asthma assessment, see your GP in person. Telehealth is appropriate for stable, established asthma requiring repeat prescriptions or routine medication review.
How much do asthma medications cost with the PBS?
From 1 January 2026, most PBS medicines cost up to $25 for general patients and $7.70 for concession card holders before the PBS Safety Net. Private prescriptions, brand premiums, and non-PBS medicines can cost more.
Can telehealth doctors diagnose asthma?
Asthma diagnosis usually requires spirometry or other in-person assessment that cannot be completed through telehealth alone. If you have not been diagnosed with asthma before, you need an in-person GP or specialist assessment.
InstantMed Medical Team
Related Articles
8 min read
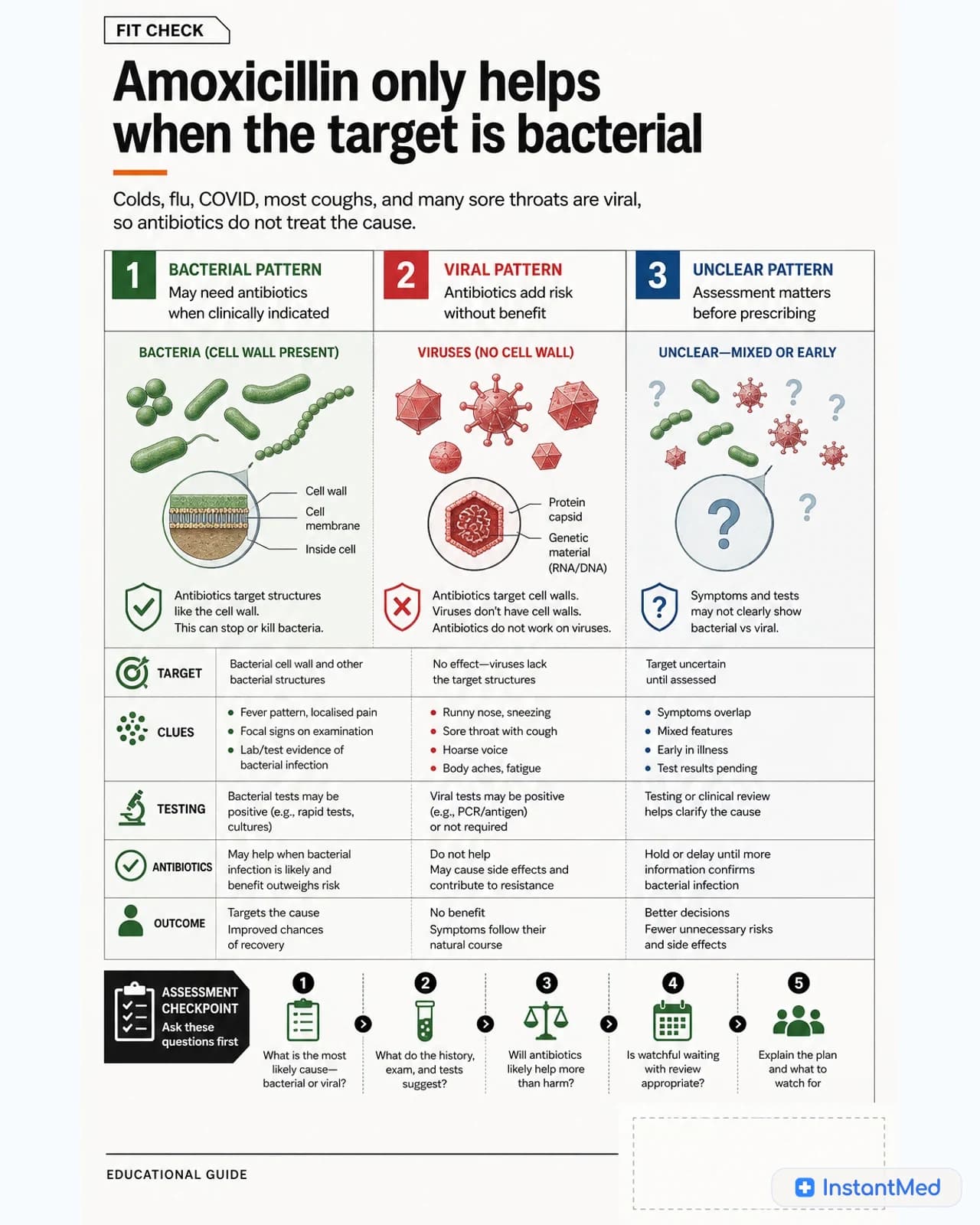
Amoxicillin in Australia: Uses, Dosing, and What to Know
Amoxicillin is a penicillin antibiotic used for selected bacterial infections. It does not treat viruses, and the right dose depends on the infection, person, and clinical context.
InstantMed Medical Team

8 min read
When Antibiotics Are Appropriate: Bacterial vs Viral Infections
Antibiotics treat bacterial infections, not viruses. This guide explains when antibiotics may be appropriate, when they are usually avoided, and what responsible use looks like.
InstantMed Medical Team

11 min read
Can You Get Antibiotics Online in Australia?
Antibiotics are prescription-only in Australia. Learn how online prescribing works, when a pharmacist can help with a UTI, what PBS costs in 2026, and which symptoms need in-person care.
InstantMed Medical Team