Loading article
Back to Health Guides
Telehealth vs GP: An Honest Comparison
When remote care is useful, when your regular GP is safer, and why the best answer is often using both for different jobs.
12 min read
·Updated 8 July 2026
·Doctor Reviewed
AHPRA Verified
In this article
- 1The honest comparison
- 2When telehealth is useful
- 3When your regular GP is better
- 4Where in-person care wins
- 5What a safe telehealth service should do
Medical information only. This article is for general information and does not constitute medical advice. Treatment decisions are made by an AHPRA-registered doctor after reviewing your circumstances.
Review
InstantMed Clinical Team
Clinical governance review for guide content
Updated
8 July 2026
General information only, not personal medical advice.
Jump to section
1The honest comparison2When telehealth is useful3When your regular GP is better4Where in-person care wins5What a safe telehealth service should do6Doctors and registration7Cost and access are real, but not the only factors8Children, older adults, pregnancy, and complexity9Choose the right route10The practical answer11Related guides12Sources Used In This Guide
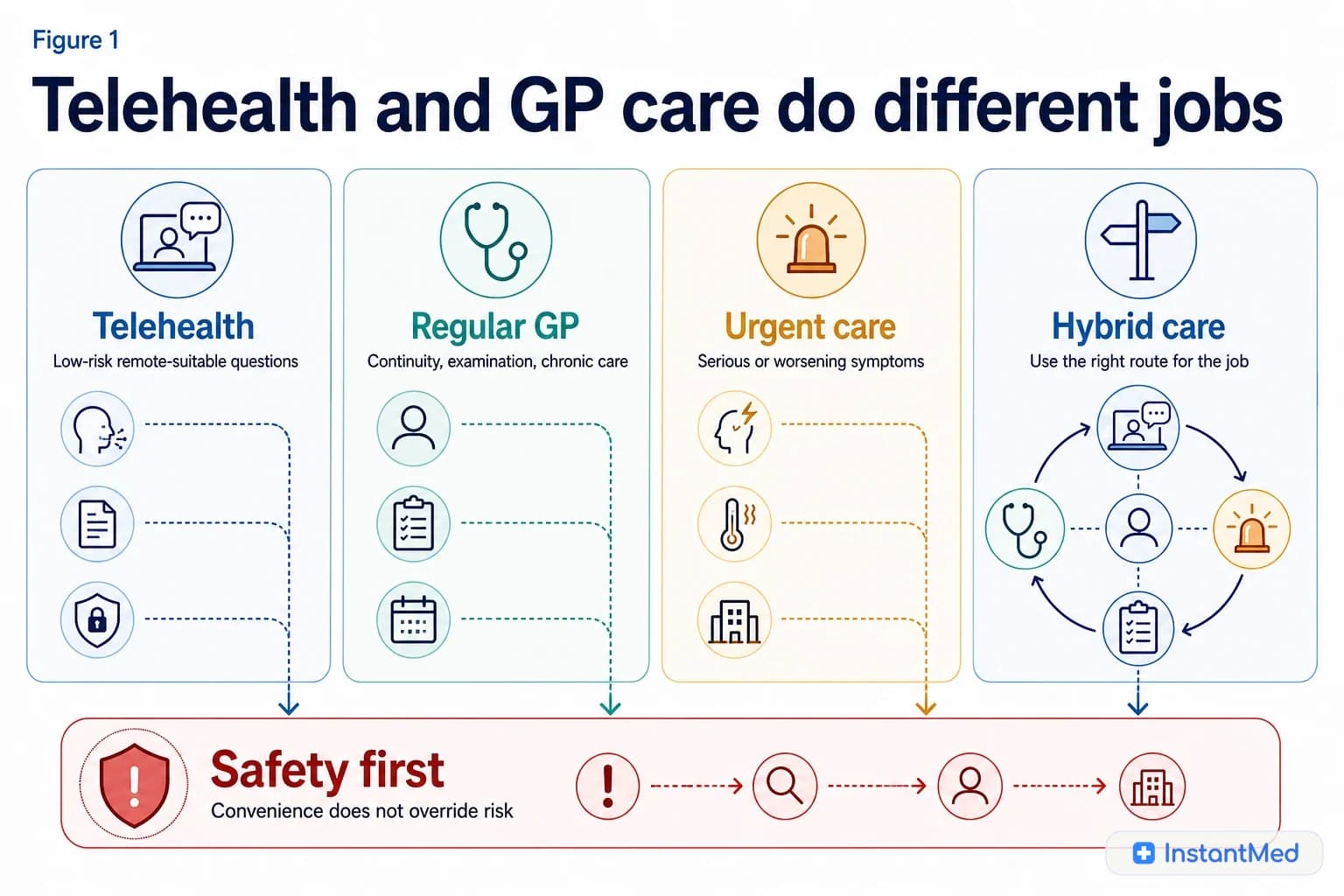
Telehealth and regular GP care are not interchangeable. They solve different problems.
Telehealth can be useful when the clinical question can be answered from history, records, images, video, or conversation. A regular GP is usually better when examination, continuity, chronic disease management, care planning, or repeated follow-up matters. Urgent symptoms should bypass both routine telehealth and routine appointments.
The honest comparison
Start by asking what the clinician needs to know to make a safe decision. If the answer depends on touch, instruments, vital signs, physical findings, pattern over time, or a care plan, a regular GP or in-person route is usually safer.
| Need | Telehealth may fit | Regular GP or in-person care may be safer |
|---|---|---|
| Clear history | Yes, when symptoms are stable and low risk | If the story is unclear, changing, or high risk |
| Physical examination | Limited | Better when chest, ear, abdomen, wound, joint, neurological, or pregnancy assessment matters |
| Tests or measurements | Can advise or arrange in some cases | Better when results must be interpreted with examination or repeated review |
| Ongoing condition | Useful for selected follow-up | Better for long-term plans, targets, reviews, and coordination |
| Medicines | May fit stable reviews | Better for new, complex, high-risk, or interacting medicines |
| Urgent symptoms | Should redirect | Urgent care, ED, or 000 may be needed |
When telehealth is useful
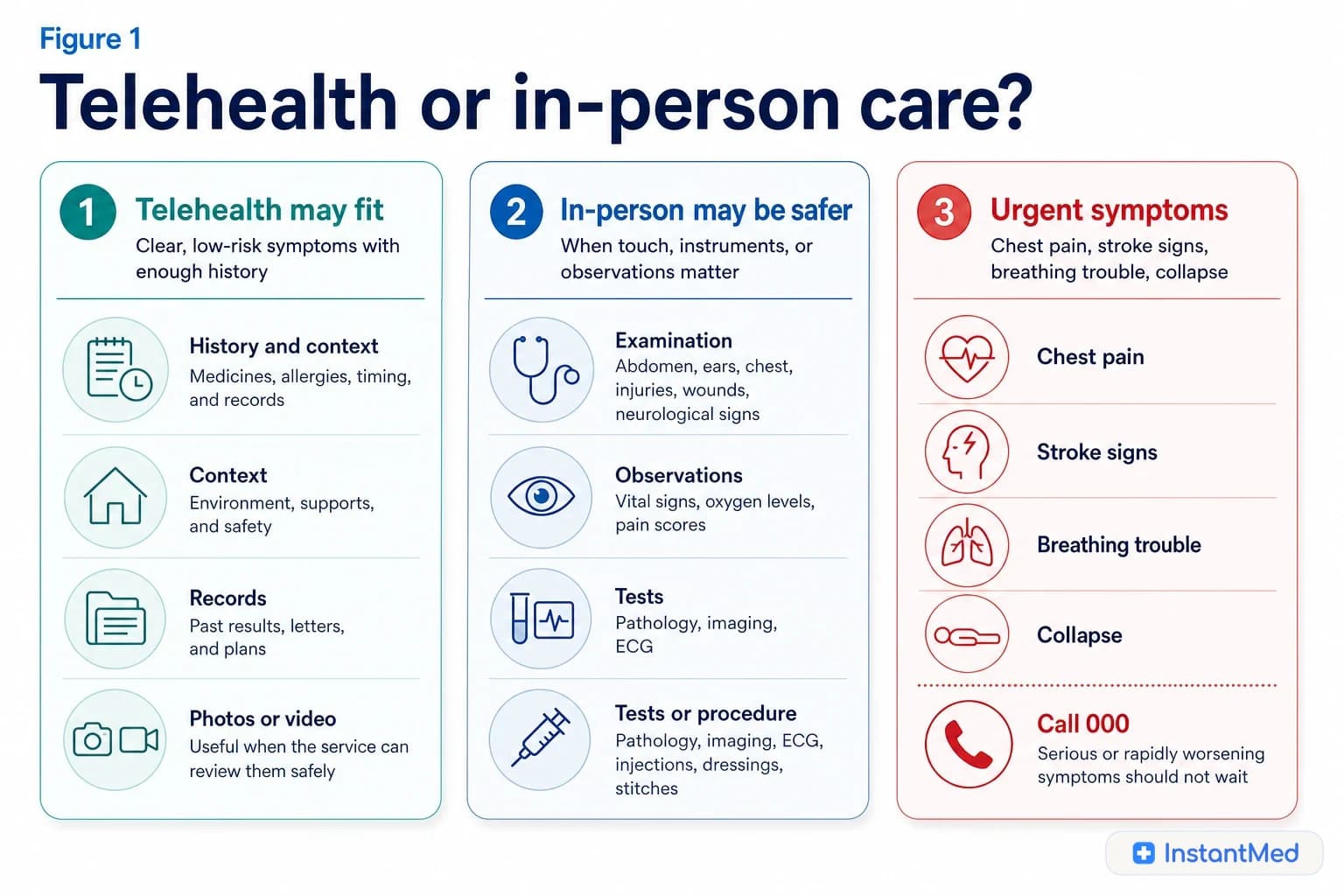
Telehealth is most useful when the problem is well-defined, low risk, and does not require a hands-on examination to make the next decision.
Examples can include:
- mild illness advice when no red flags are present
- work-capacity or certificate questions where the clinical history is enough
- follow-up after a recent in-person review where the plan is already clear
- stable medicine review where the medicine history, allergies, pregnancy status, and monitoring context are clear
- asking whether a problem needs GP, urgent care, pathology, imaging, pharmacy, or emergency care
- administrative clarification, results discussion, or advice where continuity records are available
Telehealth should also have a stopping rule. If the clinician cannot safely decide remotely, they should explain the reason and redirect you.
When your regular GP is better
Healthdirect says your GP is usually the first person to go to when you have a health concern, and that GPs can get to know you and your family over time, treat a wide range of illnesses, provide screening, give advice, and coordinate care when you have multiple health needs.
That continuity is hard to replace with one-off remote care.
| Situation | Why a regular GP often fits better |
|---|---|
| Chronic disease such as diabetes, asthma, heart disease, kidney disease, or high blood pressure | You need targets, monitoring, medicines, preventive care, and repeated review |
| Mental health care plan or long-term mental health symptoms | Care planning, risk review, referrals, and continuity matter |
| Child health concern | Examination and parent observations often need careful context |
| Pregnancy or postnatal concern | The threshold for in-person or maternity advice is lower |
| New or repeated symptom | Pattern recognition and examination may change the plan |
| Multiple medicines or specialist letters | A GP can coordinate interactions, monitoring, and records |
Where in-person care wins
Some health questions rely on information telehealth cannot collect properly.
| In-person evidence | Examples |
|---|---|
| Examination | Abdomen, ears, chest, joints, wounds, neurological signs, testicular pain, pelvic pain |
| Observations | Blood pressure, oxygen level, temperature, pulse, hydration, breathing effort |
| Procedures | Dressings, stitches, injections, ear examination, wound cleaning |
| Investigations | ECG, urine test, pathology, imaging, pregnancy-related assessment |
| Repeated review | Tracking deterioration, treatment response, or complex symptoms over time |
If you are not sure whether examination matters, telehealth may help triage. But if the clinician says examination is needed, treat that as the plan.
What a safe telehealth service should do
A safe telehealth encounter should not feel like a shortcut around medicine. It should collect enough information, check suitability, document the outcome, and redirect when needed.
Look for:
Figure 2
Examination, continuity, repeated symptoms, complex medicines, care plans, and young patients often need GP context.
| Safety checkpoint | What it means |
|---|---|
| Identity and contact details | The service knows who is being reviewed and how to contact them |
| Consent and billing clarity | You understand the remote process, limits, and costs |
| Clinical history | Symptoms, timing, severity, medicines, allergies, pregnancy status, and relevant background are captured |
| Red-flag screening | Urgent symptoms are actively checked |
| Records and follow-up | You receive clear advice, documents if appropriate, and escalation instructions |
| Redirect pathway | GP, urgent care, ED, pathology, imaging, or 000 is recommended when remote care is not enough |
Doctors and registration
All doctors practising medicine in Australia need appropriate registration. Ahpra keeps the public Register of Practitioners, including medical practitioners, and the Medical Board sets professional expectations for doctors.
The difference between telehealth and GP clinic care is usually not whether the doctor is "real". The difference is what information the doctor can safely gather in that format.
| Question | Why it matters |
|---|---|
| Is the doctor AHPRA-registered? | Registration can be checked on the public register |
| Is the clinical question remote-suitable? | Some problems need examination or tests |
| Does the service explain limits? | Safe services should name what they cannot manage remotely |
| Will my GP know what happened? | Continuity improves when records and updates are shared appropriately |
Cost and access are real, but not the only factors
It is reasonable to consider cost, travel, appointment availability, time off work, childcare, and whether you are too unwell to sit in a waiting room. Those factors are part of access.
But cost and convenience should not be the only decision factors. The cheapest or fastest route is not the right route if it cannot safely assess the problem.
| Access factor | How to think about it |
|---|---|
| Time | Telehealth can reduce travel and waiting for suitable issues |
| Cost | Compare the fee, rebate, gap, medicines, and time cost |
| Availability | If your usual GP is unavailable, telehealth may help triage or manage low-risk needs |
| Continuity | For ongoing problems, returning to the same GP can be more valuable than speed |
| Safety | Urgent symptoms should override convenience |
Children, older adults, pregnancy, and complexity
Telehealth can still be useful for selected questions in these groups, but the threshold for in-person care is lower.
Be more cautious when the patient is:
- a baby or young child
- pregnant or recently postpartum
- older, frail, immunocompromised, or medically complex
- confused, faint, breathless, dehydrated, severely unwell, or rapidly worsening
- taking multiple medicines or high-risk medicines
- in mental health crisis or immediate danger
- unable to describe symptoms clearly
If a parent, carer, or patient feels something is seriously wrong, take that seriously.
Choose the right route
Decision guide
Telehealth, regular GP, or urgent care
May fit telehealth
- The problem is stable, low risk, clearly described, and no danger signs are present.
- History, records, photos, video, or a focused conversation give enough information for a safe next step.
Needs in-person care
- Examination, observations, pathology, imaging, procedures, pregnancy assessment, child assessment, chronic disease review, or repeated follow-up may change the plan.
- Your regular GP needs to coordinate medicines, specialist letters, care plans, or long-term monitoring.
Urgent care
- Chest pain, stroke signs, severe breathing difficulty, collapse, seizure, severe bleeding, poisoning, overdose, major injury, immediate self-harm risk, or rapid worsening should bypass routine telehealth.
- Call 000 for serious and urgent symptoms.
Figure 3
Remote review works best when records, GP follow-up, and urgent redirection stay connected.
The practical answer
Use telehealth for the work telehealth handles well: low-risk remote review, triage, simple follow-up, and suitable one-off episodes. Use your regular GP for the work continuity handles well: examination, chronic care, prevention, care plans, medicines, children, mental health, and complex problems.
The strongest model is not telehealth instead of a GP. It is telehealth with a GP, with clear boundaries.
Related guides
- Telehealth vs GP in Australia
- Telehealth vs in-person doctor
- When telehealth cannot help
- How to prepare for a telehealth appointment
Sources Used In This Guide
- Australian Government Department of Health, Disability and Ageing: Telehealth
- Medical Board of Australia: Telehealth consultations with patients
- Healthdirect: The role of a GP
- Ahpra: Registers of Practitioners
- Healthdirect: Calling triple zero (000)
- Healthdirect: Mental health crisis support
Frequently Asked Questions
Is telehealth as good as seeing a GP?
For some low-risk questions, telehealth can be clinically appropriate. It is not the same as seeing a GP in person when examination, observations, tests, procedures, repeated review, or long-term context matter.
Can telehealth replace my regular GP?
No. A regular GP provides continuity, physical examination, prevention, chronic disease care, care plans, mental health planning, and coordination with specialists. Telehealth is better treated as a useful additional access route.
When is telehealth the better first step?
Telehealth may be a reasonable first step for stable, low-risk symptoms, simple follow-up questions, work-capacity or certificate questions, and medicine reviews where the history and records are enough and no urgent features are present.
When should I see a GP instead?
See a GP or in-person service when the problem needs examination, measurements, pathology, imaging, procedures, pregnancy assessment, child assessment, chronic disease review, mental health care planning, or repeated follow-up.
What if telehealth says I need in-person care?
Follow that advice. A redirect to a GP, urgent care, emergency department, pathology, imaging, or 000 is a safety feature, not a failure.
Should I tell my GP I used telehealth?
Yes, especially if a medicine, certificate, referral, test, or care plan changed. Keeping your regular GP informed supports continuity and reduces the chance of fragmented records.
InstantMed Medical Team
Related Articles

11 min read
Telehealth vs GP: What's Actually Different in Australia?
Telehealth and in-person GP care are not rivals. Telehealth can be useful for suitable remote assessment, while GP clinics remain essential for examination, continuity, procedures, tests, and complex care.
InstantMed Medical Team
12 min read
Telehealth vs In-Person Doctor: When to Use Each
Telehealth and in-person care answer different clinical questions. This guide explains when remote review may fit, when a physical examination or tests matter, and when urgent symptoms should bypass routine care.
InstantMed Medical Team

11 min read
When Telehealth Cannot Help: Knowing the Limits
Telehealth can be safe and useful when the problem fits remote assessment. It cannot replace emergency care, a physical examination, monitoring, or continuity when those are needed. This guide explains the limits and safer next steps.
InstantMed Medical Team